


Why your torn Meniscus might be normal

So you’ve developed knee pain, you’ve been sent for an MRI and there you are with the scan results in your hand. The report is telling you that your knee has a range of abnormal findings including a meniscus tear. Uh oh! This must be why your knee hurts…well maybe not. The reality is that this tear may have been there long before the knee pain existed.
MRI Findings
Often scan findings are linked to a person’s cause of pain however this relationship between knee pain and abnormal MRI results is not always precise. Not only meniscus tears but cartilage defects, bone marrow lesions, osteophytes and other features of osteoarthritis can be commonly found on knee scans (2). It’s never been more important that scans must be interpreted with caution. We now have unprecedented access to imaging services with over 27,000,000 medical imaging investigations occurring annually in Australia. This costs Medicare a whopping $4 billion yearly (1).
So what are the facts?
A large review study published in 2018 looked at 3761 knees in people who were pain free. From a collection of 44 studies this is what they found:
- On average, 10% of pain free knees had a meniscal tear
- 4% of people younger than 40 years old had a tear
- 19% of people 40 years or over had a meniscus tear (2)
Just recently another study looked at both knees of 115 uninjured, pain free volunteers (that’s 230 knees total). This study used an even stronger MRI machine (3.0T) than previous studies and what they found was:
- 30% of pain free knees had a meniscus tear
- A further 18% had meniscus degeneration
- Therefore 48% of asymptomatic volunteers had an abnormal meniscus (3)

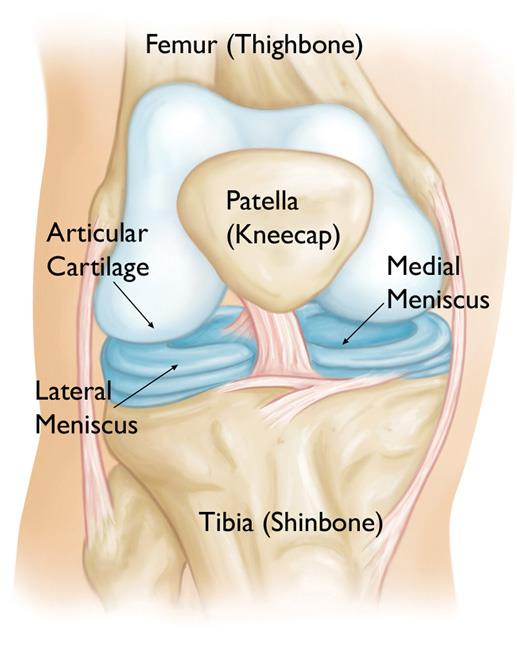
Anatomy of the knee joint
Should I get a scan?
The answer to this isn’t a straight forward yes or no but there should be a good reason to send someone for a scan. Guidelines were developed to prevent unnecessary knee radiographs following knee trauma, these are called the Ottawa Knee Rules (7). The indications for a x-ray are as follows:
- aged 55 years or over
- tenderness at the head of the fibula
- isolated tenderness of the patella
- inability to flex knee to 90 degrees
- inability to bear weight (defined as an inability to take four steps, ie. two steps on each leg, regardless of limping) immediately and at presentation to a health professional
If the knee pain is from a non-traumatic incident then imaging is likely not needed unless the health practitioner is concerned about other factors such as malignancy or infection. Often a diagnosis and management plans can be developed successfully without the need for any imaging. MRI should only be considered when the knee injury diagnosis is doubtful, difficult and complex (8).

Areas of pain that warrant an X-ray post knee trauma
What about surgery?
I’ve recently written an extensive blog covering this topic titled “Meniscus Tear: Do I need Surgery?”, read it HERE>>. In that blog I take a deep dive into the current body of scientific evidence and unpack what we have learnt about meniscal tear surgeries.
To make a long story short, we have begun to realise that for the most part people often do not require surgery when they have damaged their meniscus. When the evidence is stacked up, the picture is quite clear that most people do just as well with structured physiotherapy. Three metanalyses published between 2014 to 2018 all concluded that in longer term follow ups (greater than 6 months) surgery had no benefit over exercise therapy (4,5,6). Yet 4 million meniscal debridement’s occur per year worldwide.
So what does this mean for you?
Just because you have abnormal findings on a scan does not mean it’s the cause of your knee pain. Let me repeat that, we can’t determine someone’s pain source purely from a scan. This is where it is important to always match a person’s clinical history with their medical imaging – and this is what good health practitioners do! Chances are that some of those scan findings were probably there long before your pain existed.
This also means that just because you have an abnormal finding on a scan, you will not always necessarily suffer pain. If 10%-30% of people can walk around with a torn meniscus and be pain-free then why can’t you. The older you get the more likely you are to have an asymptomatic meniscal tear.
Summary
- The relationship between knee pain and MRI results is not always precise
- A large review found that in on average 10% of asymptomatic people had a meniscus tear. This grew to 19% in over 40’s
- In 2020, a new study found 30% of pain-free people had a meniscus tear
- 3 large reviews found that people will do just as well with physiotherapy than surgery
- Just because you have a torn meniscus on MRI, doesn’t mean you will always experience pain from it

James Gardiner
POGO Physiotherapist
Book an Appointment with James here.
Featured in the Top 50 Physical Therapy Blog
References
- Australian Government. (2020, March 12). Annual Medicare statistics. Department of Health. https://www1.health.gov.au/internet/main/publishing.nsf/Content/Annual-Medicare-Statistics
- Culvenor, A. G., Øiestad, B. E., Hart, H. F., Stefanik, J. J., Guermazi, A., & Crossley, K. M. (2018). Prevalence of knee osteoarthritis features on magnetic resonance imaging in asymptomatic uninjured adults: A systematic review and meta-analysis. British Journal of Sports Medicine, 53(20), 1268-1278.
- Horga, L. M., Hirschmann, A. C., Henckel, J., Fotiadou, A., Di Laura, A., Torlasco, C., D’Silva, A., Sharma, S., Moon, J. C., & Hart, A. J. (2020). Prevalence of abnormal findings in 230 knees of asymptomatic adults using 3.0 T MRI. Skeletal Radiology.
- Rogers, M., Dart, S., Odum, S., & Fleischli, J. (2019). A cost-effectiveness analysis of isolated Meniscal repair versus partial meniscectomy for red-red zone, vertical Meniscal tears in the young adult. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 35(12), 3280-3286.
- Khan, M., Evaniew, N., Bedi, A., Ayeni, O. R., & Bhandari, M. (2014). Arthroscopic surgery for degenerative tears of the meniscus: A systematic review and meta-analysis. Canadian Medical Association Journal, 186(14), 1057-1064.
- Lee, D., Park, Y., Kim, H., Nam, D., Park, J., Song, S., & Kang, D. (2018). Arthroscopic meniscal surgery versus conservative management in patients aged 40 years and older: A meta-analysis. Archives of Orthopaedic and Trauma Surgery, 138(12), 1731-1739.
- Stiell, I. G. (1996). Prospective validation of a decision rule for the use of radiography in acute knee injuries. JAMA: The Journal of the American Medical Association, 275(8), 611.
- Clinical guidance for MRI referral. (2013). RACGP – The Royal Australian College of General Practitioners. https://www.racgp.org.au/FSDEDEV/media/documents/Clinical%20Resources/Guidelines/MRI/Summary-sheet-%e2%80%93-MRI-of-the-knee-for-meniscal-and-anterior-cruciate-ligament-tears.pdf








Good post. Interesting I read about the asymptomatic tears before. I supposedly tore my meniscus two times according to the MRI however I always wondered if it was the same tear as the first because it was in the same place.
Surgery does sound to be overly recommended and the results of excision do not look good for many. Repair or stitches looks better, but most of the time I would try to heal it naturally before doing any surgery. Either way you should do rehab on it and don’t expect it to return to normal without any effort. Maybe but I doubt it. Or expect the doctor to “fix it”.
There are other treatments you can too that are more natural.