Scheuermann’s Disease

Scheuermann’s disease (also known as Scheuermann’s kyphosis) is a rigid deformity occurring due to wedging of thoracic vertebrae during the rapid stages of spinal growth (1). Scheuermann’s Disease was first described by Holger Werfel Scheuermann in 1920 (2). In 1964, Sorensen was the first to define the condition radiographically by the presence of at least three adjacent vertebrae wedged a minimum of five degrees (2).
Aetiology:
Scheuermann’s Disease is broadly thought to be idiopathic (Unknown cause) in its origin (1).
Scheuermann himself believed that osteonecrosis (bone cell death) of the vertebral ring apophysis resulted in longitudinal growth arrest of the anterior vertebral body, thus causing a wedging of the vertebrae (2). Schmorl postulated that disk material herniated through the vertebral end plates lead to loss of disk height, vertebral body wedging, and node formation (2).
Both these early theories have since been called into question – a genetic pattern of inheritance of the condition is now accepted, with evidence of increased prevalence in twins (1). The pattern of inheritance is thought to be autosomal dominant with variable penetrance (1). There is no clear gender predominance for the condition, although some studies report a higher incidence in males (1).
Epidemiology:
- Prevalence: 1% to 8% in the United States
- Sex: Male to female ratio is at least 2:1
- Age: Most commonly diagnosed in adolescents 12-17 years
- Rarely diagnosed in children less than 10 years.
- Classification:
- Type I (Classic) – Thoracic spine involvement only, with the apex of curve T7-T9
- Type II – Thoracic and lumbar involvement, with the apex of curve T10-T12 (4)
Symptoms:
- May have local tenderness around the deformity
- Tightness of hamstrings/ hip flexor muscles
- Stiff anterior shoulders
- Pain appears to be most severe in adolescence (reported by 50% of patients) and becomes less common once spinal growth is complete (reported in only 25% of adult patients)
- Patients with larger curves can progress as adults and develop disabling back pain, degenerative spondylolysis, disc herniation and neurological complications (1,2)
How is it Diagnosed?
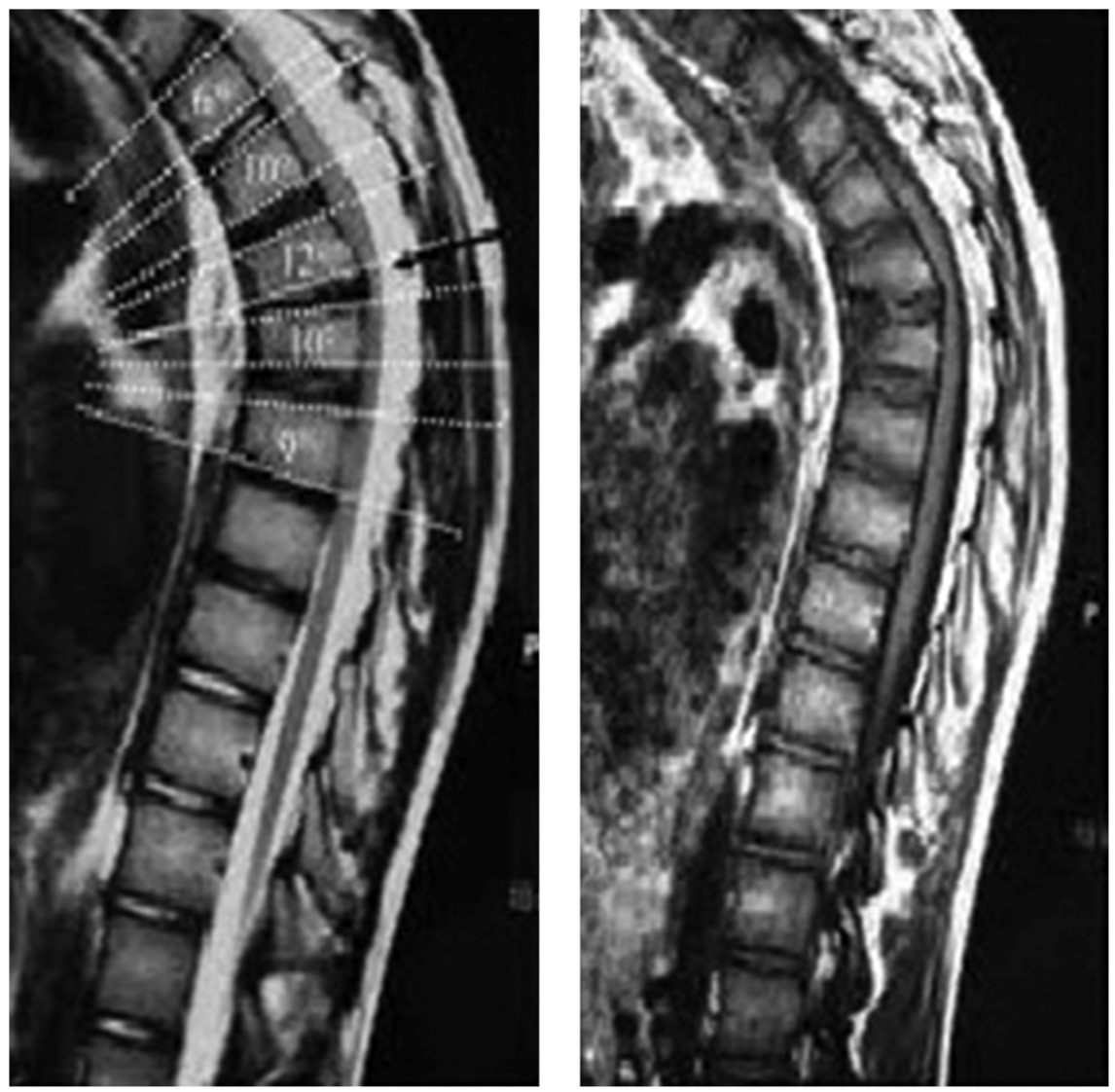
To diagnose Scheuermann’s Disease – requires a relevant history (see cause/epidemiology/symptoms above) and x-ray imaging of the lateral thoracic spine showing five degrees anterior wedging at three or more vertebrae at the apex of the curve and an overall thoracic kyphosis more than 45 degrees (1).
Other conditions that can present similarly to Scheuermann’s that should be ruled out prior to diagnosis include:
- Postural kyphosis (flexible postural deformity)
- Hyperkyphosis attributable to another known disease state
- Postsurgical kyphosis
- Ankylosing spondylitis
- Scoliosis (4)
The natural history of Scheuermann’s disease is currently unclear. There is a lack of data on the long-term follow-up of both untreated and surgically treated patients for any (1). From the research that has been conducted – The natural history of the condition tends to be benign (not harmful in effect) (2). In patients with a smaller degree of kyphosis (less than 60), good clinical outcomes can be expected (2). Only in patients with severe kyphosis of greater than 100 was lung function affected negatively neurologic complications have been reported in a small number of patients (2)
Management Pathways
Physiotherapy
Physiotherapy aims to increase strength and endurance in the trunk extensors and improve global spinal balance and posture (1,2). Hamstring tightness, core stability and shoulder/neck stiffness should also be considered and addressed in the exercise programme (1). Treatment is recommended for patients with smaller, flexible curves and can be used as an adjunct to bracing to prevent stiffness. There is no evidence as yet that physiotherapy can prevent curve progression, but pain levels may be improved (1).
Bracing
Traditional indications for bracing include a flexible kyphosis in a skeletally immature patient that is less than 65 degrees and corrects by 15 degrees on initiation of brace treatment (1). Results are less predictable with stiff curves, curves over 65 degrees and in skeletally mature patients (1). However, control of the kyphosis can be observed in curves up to 75 (1). Bracing may have a role in the treatment of smaller, flexible curves but this is likely to only prevent progression rather than correct the curvature. (1)Overall there is a paucity of data to support bracing treatment of Scheuermann’s disease, and the effect of bracing treatment on the natural history and progression of disease remains unknown (2).
Surgical Treatment
Surgical treatment of Scheuermann’s disease is reserved/indicated for patients with one or more of the following:
- Greater than 70-75 degree thoracic curves
- Greater than 25-30 degree thoracolumbar curves
- Intractable pain
- Neurological deficit
- Cardiopulmonary compromise
- Poor cosmesis (appearance) (1,2)
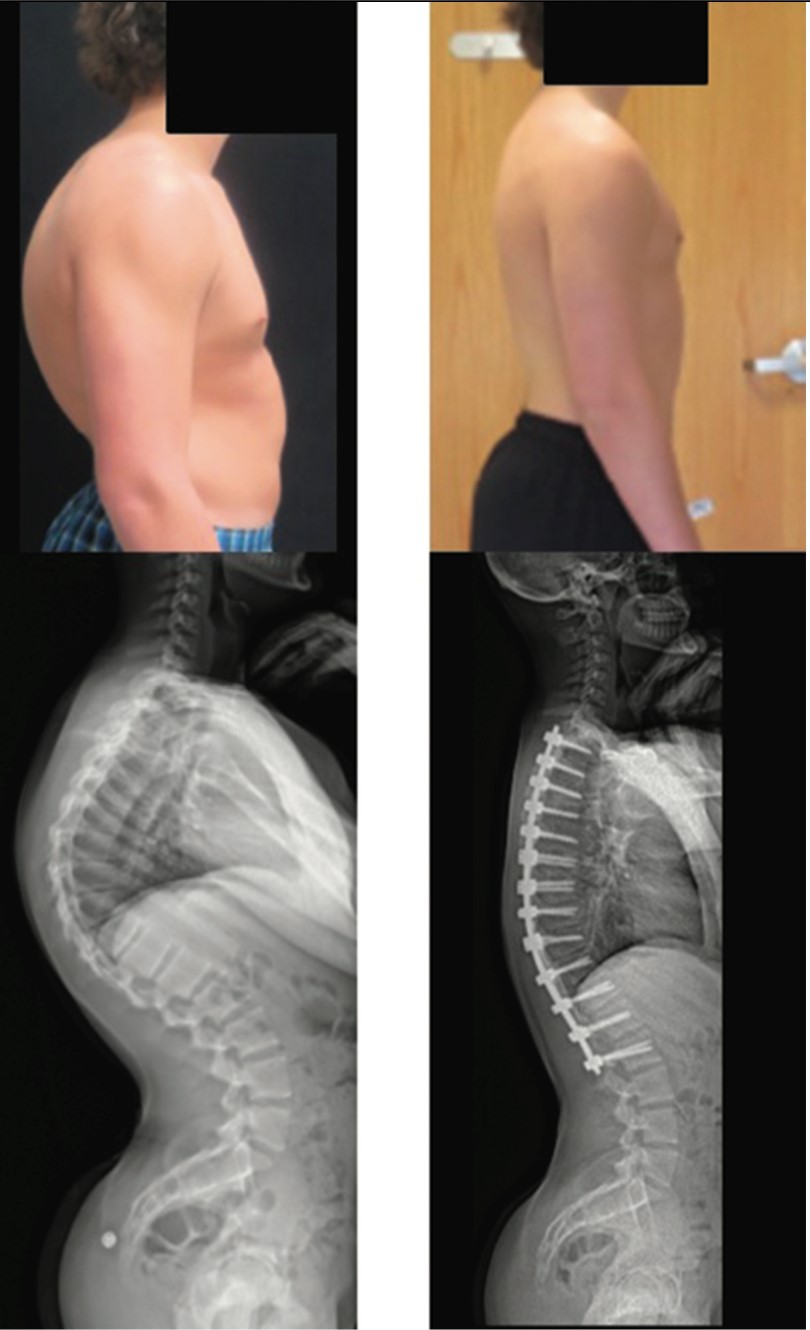
Uncertainty over the natural history of Scheuermann’s makes it difficult to identify clear reasons for surgical intervention (1). Surgery is typically performed in adolescents for progressive deformities over 70 degrees that are associated with pain and have not responded successfully to nonoperative treatment (analgesia, change of activities, physiotherapy and bracing) (1).The anticipated benefits of surgery must be balanced with the risks of surgery and discussed with the patient and their family (1).
New surgical procedures for Scheuermann’s disease permit improved correction of the deformity via posterior surgery with lesser complication rates (3). Concurrent shortening of the posterior spinal column crossways the apical levels, and combined by monitoring of spinal cord, decreases the danger of neurological deficits (3). Kyphosis correction has been associated with reduction in back pain and high rates of patient satisfaction but also with a high risk of complications (1).
Consult a Medical Professional or Physiotherapist for proper diagnosis/management of this condition. If you’re on the Gold Coast – come in and see us at POGO Physio!

Oliver Crossley (APAM)
POGO Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References
- Loughenbury, Peter R., and Athanasios I. Tsirikos. “Scheuermann’s kyphosis: diagnosis, presentation and treatment.” Orthopaedics and Trauma 31, no. 6 (2017): 388-394.
- Sardar, Zeeshan M., Robert J. Ames, and Lawrence Lenke. “Scheuermann’s Kyphosis: Diagnosis, Management, and Selecting Fusion Levels.” The Journal of the American Academy of Orthopaedic Surgeons (2018)
- Haddadi, Kaveh, Abhijeet Kadam, Chadi Tannoury, and Tony Tannoury. “Scheuermann’s Disease: New Impressions of Clinical and Radiological Evaluation and Treatment Approaches; A Narrative Review.” Journal of Pediatrics Review 6, no. 2 (2018): 37-45
- Mansfield, J. T., and Matthew Bennett. “Scheuermann Disease.” (2018).