Common Causes of Elbow Pain: Diagnosing and Understanding Symptoms

Elbow pain is a common issue that can arise from various causes, often limiting mobility and affecting daily functions. Elbow pain can present as an acute incident, gradual onset or occasionally an acute moment increasing mild pre-existing symptoms. This article will explore common causes of elbow pain and discuss the typical signs, symptoms, and characteristics of these conditions, as well as some implications for management.
Anatomy
The Elbow is a hinge joint located between the upper arm and the forearm. The elbow joint plays an essential role in upper limb mobility and function, allowing for precise and coordinated movement of the upper limb, particularly the wrist and hand. The movements of the elbow joint include flexion and extension (bend and straightening) and supination and pronation (palm up and palm down, respectively). The elbow joint is formed by the articulation of three bones:
- Humerus: The upper arm bone that extends from the shoulder to the elbow.
- Radius: The larger of the two forearm bones, located on the thumb side of the arm. It plays a key role in wrist and elbow movements, especially in pronation and supination (rotation).
- Ulna: The longer of the two forearm bones, located on the pinky side of the arm. The ulna is the main bone involved in elbow flexion and extension.
Together with the local ligaments these bone form three distinct joints;
- Humeroulnar Joint: A hinge joint between the humerus and ulna, responsible for most of the elbow’s flexion and extension.
- Humeroradial Joint: The articulation between the humerus and radius, facilitating both flexion and extension as well as limited rotation.
- Proximal Radioulnar Joint: Where the radius and ulna meet near the elbow, allowing for pronation (turning the palm down) and supination (turning the palm up).
For ease in thinking about the differential causes, signs and symptoms of elbow pain here let’s separate the areas of pain into anterior (front), posterior (back), medial (inside – closest to the body) and lateral (outside) causes. As the same location of pain with different onset (acute vs gradual) will often have different diagnoses we will consider these separately.
Anterior Elbow Pain – Acute Onset:
Distal Biceps Tear: A tear of the distal biceps tendon occurs with a sudden, sharp pain in the front of the elbow, particularly during activities involving lifting or pulling. It is often described as a pop or letting go sensation.
Diagnostic Tests
- Hook Test: A positive test (where the examiner cannot hook their finger under the biceps tendon) can indicate a tear. While the test’s negative result does not exclude a tear, a positive test in chronic cases may suggest the need for surgical intervention.
- Biceps Crease Interval Test: If the distance between the biceps tendon’s flexion crease and the biceps divergence line is greater than 6 cm, this may signal a tear.
- The combination of both tests offers higher accuracy in diagnosing distal biceps tears (Zwerus et al., 2018).
Signs and Symptoms:
- Sudden sharp pain at the front of the elbow
- Visible deformity (often called the “popeye sign” where the biceps muscle bulges)
- Weakness in elbow flexion and supination
- Higher incidence in smokers and steroid users
Loose Bodies: Loose bone fragments due to avulsion or previous existing injury can lock and present with anterior pain
Capsular Injury: A stretching or hyperextension injury that results in a stretch to the anterior aspect of the elbow joint capsule.
Anterior Elbow Pain – Gradual Onset:
Distal Biceps Tendinopathy: A change in structure to the biceps tendon due to overload of the biceps. Presents with localised pain to the biceps insertion on the tendon and pain with elbow flexion and supination. Management is primarily in reducing bicep loads, supporting shoulder and kinetic chain strength and control then progressive strengthening or reloading biceps brachii.
Signs and Symptoms:
- Pain and tenderness at the front of the elbow with gripping or lifting activities
- Weakness in forearm supination
- Limited elbow extension
- Sudden or recent increase in biceps training loads
Pronator Teres Syndrome: Pronator teres is a long muscle of the forearm that pronates the wrist (turns palm down). Compression of the median nerve at the pronator teres muscle results in pain and sensory disturbances in the forearm along the path of the medial nerve
Signs and Symptoms:
- History of increased load of pronation activities (climbers, chin ups and pull ups at higher loads)
- Pain on resisted pronation particularly with elbow extension
- Tinel’s test positive – tapping on path of median nerve
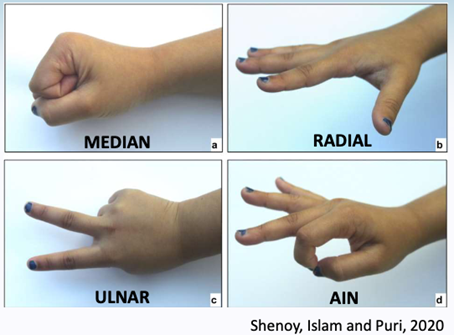
- As it innervates flexor pollicis longus and flexor digitorum profundus a weaker ‘OK’ sign (thumb to first finger push)

Radial Tunnel Syndrome: Compression of the radial nerve, leading to pain and weakness in the forearm and hand. This is discussed more below in lateral elbow pain.
Osteochondritis Dissecans (OCD): A condition where the bone and cartilage in the elbow joint become damaged, leading to gradual pain and limited range of motion. This is most common in adolescents but can lead to loose bodies in older adults.
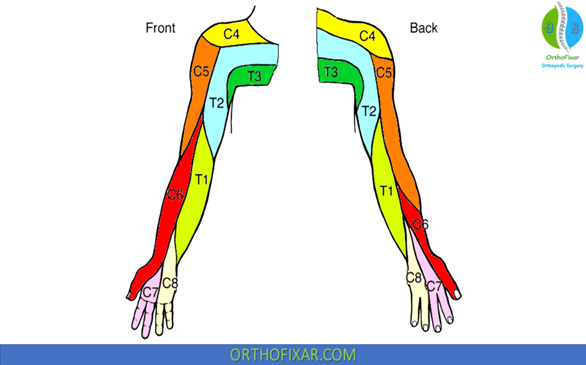
Radiculopathy (C5/6): Elbow Pain can be the result of referred pain from the neck at the level of the C5 or C6 nerve root. Elbow pain can be accompanied by neck pain and/or upper arm pain, hand pain (5th digit) or sensory changes (pins and needles, numbness).
Medial Elbow Pain – Acute Onset:
Ulnar Collateral Ligament (UCL) Sprain: Often seen in athletes, especially in throwers and baseball pitchers, this ligament injury can cause sharp pain on the inside of the elbow.
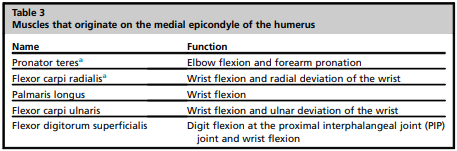
Common Flexor Origin Injury: The common flexor origin is the tendon attachment point for multiple flexors of the wrist and hand. AN acute moment that overloads the wrist into resisting flexion, gripping or forearm rotation can lead to partial tear or rupture of medial elbow tendon. This often can be on the background of medial elbow tendinopathy or previous medial elbow pain.
Loose Bodies: These can occur after injury, causing pain and mechanical symptoms such as locking or catching of the elbow.
Medial Elbow Pain – Gradual Onset:
Medial Epicondylalgia or Medial Elbow Tendinopathy (Golfer’s Elbow): Painful tendon or tendons on the inside of the elbow, often caused by an increased amount of repetitive wrist flexion and forearm rotation.
Signs and symptoms
- Pain 1-2 cm below medial epicondyle
- Overload – badminton, squash, tennis or golf or manual labour.
- Can occur after large, sudden forceful movements including heavy lifting or gripping force through the arm
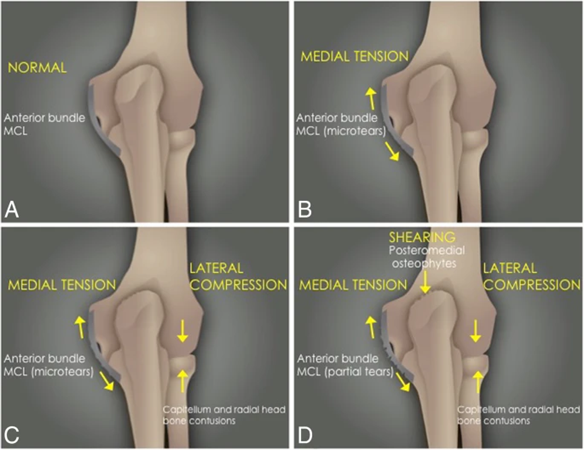
Medial Instability: Medial pain as a result of increased laxity or hypermobility medially or difficulty controlling medial forces. Most common among gymnasts and throwers or the younger upper limb athlete. These can occur subtly with the growth plate still not fusing until 17 years of age. Some consequences or medial instability can be compression laterally at the radiohumeral joint posteromedial olecranon compression and can lose terminal extension as illustrated below.
Medial Impingement: A condition where the structures of the elbow joint (often medially) are often associated with osteoarthritis contact against each other, leading to pain and decreased range of motion. This can be related to local arthritis (osteoarthritis or inflammatory) or previous trauma. There can be pain and restriction of range of movement as impingement occurs at the extremities of range of motion. Can be associated with morning elbow stiffness.
Ulnar Nerve Neuropathy: Compression or irritation of the ulnar nerve as it passes through the cubital tunnel, causing numbness, tingling, and weakness in the hand. A quick test for damage to the ulnar nerve or other nerves include can you make the shapes below. Ulnar nerve neuropathy can occur as a consequence of other diagnosis or injury such as medial instability. Neural tension tests for the ulnar nerve are often provocative.
Radiculopathy (C8-T1): Nerve compression or irritation in the cervical spine can refer to pain in the medial side of the elbow.
Posterior Elbow Pain – Acute Onset:
Triceps Tear: A rupture of the triceps tendon at the back of the elbow is typically caused by sudden, forceful extension of the arm. This is followed by significant loss of power in extending the elbow.
Olecranon Bursitis: Inflammation of the bursa at the back of the elbow can result from repetitive pressure or trauma, often seen in those who lean on their elbows frequently. Swelling and increased size of the bursa is easily seen at the back of the elbow.
Fractures: An olecranon or radial head fracture can cause severe pain and swelling at the posterior elbow. Often this is a result of a fall onto an outstretched arm with the elbow moving into extension and compression or hyper-extension. Stress fractures can also occur in this location due to repetitive elbow loading into extension or hyperextension or impact loads.
Loose Bodies: Small fragments of bone or cartilage in the joint can cause irritation and pain during movement.
Posterior Elbow Pain – Gradual Onset:
- Triceps Tendinopathy: Chronic overuse or microtrauma to the triceps tendon can lead to pain at the back of the elbow. Pain on activities such pushing up out of a chair, narrow push ups and other tricep loading exercises.
- Osteochondritis Dissecans (OCD): A gradual deterioration of the bone and cartilage at the back of the joint.
- Posterior Impingement: Occurs when the structures at the back of the elbow (olecranon) abut against the humerus during extension.
- Posterolateral Instability: See below
Lateral Elbow Pain – Acute Onset:
Posterolateral Rotatory Instability: This condition involves a dislocation or subluxation of the radial head and can lead to pain and instability in the lateral elbow.
Signs and symptoms:
- Instability from acute lateral traumatic episodes (into valgus) or repeated microtrauma leads to radial head subluxation forward and backward. Giving way when weight bearing especially when moving into extension (eg push up).
- Pain with throwing activities
- Pain during the following, then relieved by relocation tests of radial head with elbow extension during increasing level of loading;
‣ Tabletop relocation (low body weight loads)
‣ Chair Sign (medium stress)
‣ Active push (higher stress)
Fracture of Radial Head/Neck: A direct blow to the elbow or fall onto an outstretched arm can cause a fracture, leading to lateral elbow pain.
Lateral Elbow Pain – Gradual Onset:
Lateral Epicondylalgia (Tennis Elbow): This is one of the most common causes of lateral elbow pain, resulting from the overuse of the extensor tendons of the forearm. 3% of the general population get Lateral Epicondylalgia, 40% of tennis players and common in trade populations and paddlers.
Signs and symptoms:
- Localised tendon pain 1-2 cm distal to lateral epicondyle
- Aggravated by 3rd digit extension (using the ECRB tendon) (positive Maudsley’s Test)
- Aggravated on wrist extension (positive cozen’s test)
- Gripping pain (grip weakness and increase in pain in elbow extension versus flexion)
- Pain on resisted pronation
- Less common in those under 30
- Partial tears less likely relevant in those older than 35 years
- Can occur alongside radial nerve sensitivity
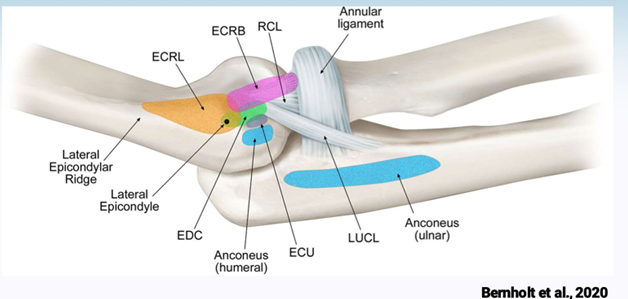
Posterior Interosseous Nerve Entrapment/Radial Tunnel Syndrome: Compression of the radial nerve in the forearm, causing pain on the lateral side of the elbow and weakness in the forearm. The common site of entrapment is where the deep motor branch of the radial nerve called the posterior interosseous nerve pierces the supinator muscle.
Signs and symptoms:
- Diffuse aching forearm pain over extensors muscles and even down into the hand
- Rarely sensory or motor changes – but can cause thumb weakness into extension and abduction
- Worse at night
- Pain increased by resisted supination, nerve palpation and or radial nerve neurodynamic tests
- Potential compression on US imaging
- Electrodynamic testing often inconclusive
Osteochondritis Dissecans (OCD): A condition where the cartilage and bone at the lateral elbow (typically the capitellum) deteriorate over time due to repetitive stress.
Irritation of the radio-capitellum synovium or bursa
Radiculopathy
Plica Syndrome
Paediatric Elbow Injuries
Children, especially those involved in sports, are prone to specific elbow injuries. In particular, fractures and dislocation are much more common. Fracture or dislocation typically occurs with a fall from height (trampoline, playground, horse, or gymnastics) or fall on outstretched hand (FOOSH). These injuries often require careful management to avoid long-term complications with the location of the fracture and degree of displacement varying management (surgery or immobilization/bracing followed by physiotherapy). The adolescent medial elbow pain can be a result of previously mentioned OCD or medial growth plate (apophysitis) termed little league elbow.
Summary
Elbow pain can result from a wide range of conditions that affect different areas of the joint. Whether from acute injuries like fractures or tears, or gradual conditions like tendinopathies, instability or nerve entrapments, understanding the specific location, history, signs and symptoms and combined with a thorough clinical assessment will enable the clinician to determine an accurate diagnosis. This is then combined with further assessment of impairments (ROM, strength, endurance, proprioception) and contributing factors to determine appropriate management.

Lewis Craig (APAM)
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References
- Coombes, B. K., Bisset, L., & Vicenzino, B. (2015). Management of lateral elbow tendinopathy: one size does not fit all. Journal of orthopaedic & sports physical therapy, 45(11), 938-949.
- Vij N, Kiernan H, Miller-Gutierrez S, Agusala V, Kaye AD, Imani F, Zaman B, Varrassi G, Viswanath O, Urits I. Etiology Diagnosis and Management of Radial Nerve Entrapment. Anesth Pain Med. 2021 Feb 14;11(1):e112823. doi: 10.5812/aapm.112823. PMID: 34221946; PMCID: PMC8236840.
- Zwerus EL, Somford MP, Maissan F, Heisen J, Eygendaal D, van den Bekerom MP. Physical examination of the elbow, what is the evidence? A systematic literature review. Br J Sports Med. 2018 Oct;52(19):1253-1260. doi: 10.1136/bjsports-2016-096712. Epub 2017 Mar 1. PMID: 28249855.